 |
Clinical Image
A midway to disaster: Concealed pneumomediastinum after endobronchial catheter intubation
1 Department of Anesthesiology, National Taiwan University Hospital, No. 7, Chung Shan S. Rd. (Zhongshan S. Rd.), Zhongzheng Dist., Taipei City, Taiwan (R.O.C.)
Address correspondence to:
Ya-Jung Cheng
Department of Anesthesiology, National Taiwan University Hospital, No. 7, Chung Shan S. Rd. (Zhongshan S. Rd.), Zhongzheng Dist., Taipei City 10002,
Taiwan (R.O.C.)
Message to Corresponding Author
Article ID: 100061Z12YL2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Li Y-T, Shih P-Y, Cheng Y-J. A midway to disaster: Concealed pneumomediastinum after endobronchial catheter intubation. J Case Rep Images Surg 2019;5:100061Z12YL2019.ABSTRACT
No Abstract
Keywords: Pneumothorax, Thoracoscopy/VATS, Tracheal carina, Tracheal injury
Case Report
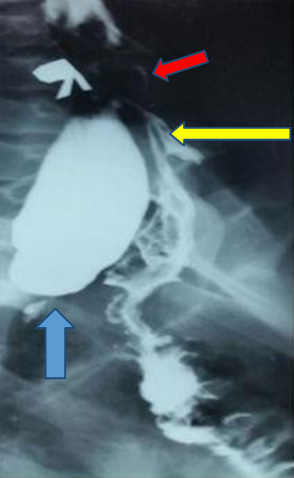
A 58-year-old woman with non-small cell lung cancer accepted right-sided video-thoracoscopic wedge resection surgery. A left-sided 35 French/Ch MallinckrodtTM double lumen endobronchialtube (DLT) with stylet was inserted smoothly, and confirmed by auscultation and fiberoptic bronchoscopy. Mild hypotension (BP: 85/60 mmHg) was found while turning her left decubitus without changes on ventilation pressure. After artificial pneumothorax, pneumomediastinum with concealed numerous widespread air bubbles was noted immediately by thoracoscopic view directed to apical chest wall (Figure 1). The blood pressure returned to normal once the mediastinum was opened to release the air. A shallow “V-shaped” laceration (arrow heads) was noted in the carina (C) by repeated bronchoscopic examination (Figure 2). The DLT was extubated smoothly after the video-assisted thoracic surgery (VATS) right middle lobe wedge resection. The following X-ray two hours later showed significant pneumomediastinum and “left” pneumothorax (Figure 3). The patient was admitted to intensive care unit for one night without any discomfort, and was discharged five days after the surgery.



Discussion
Double lumen endobronchial tube is a common instrument in thoracic surgeries. The estimated incidence of tracheobronchial rupture was reported approximately 0.3%, and was higher in women [1],[2]. Previous reports demonstrated that most common ruptured sites are distal trachea and posterior membranous wall of main bronchi [3].
Small, negligible laceration by a smooth endobronchial catheter intubation with routine fiberoptic bronchoscope could lead unpreventable injury. Without signs of tension pneumothorax, severe, concealed pneumomediastinum could be fatal by undetected cardiac tamponade effect. In this case, unexplained hypotension is the only clinical symptom. In clinical practice, accidental tracheobronchial injuries following endobronchial catheter insertion remain unpreventable. An unexplained intraoperative hypotension may be a surrogate for a tracheobronchial injury and it may be the midway with a concealed pneumomediastinum heading to disaster tension pneumothorax. Transthoracic or transesophageal echography (TTE or TEE), if available, may provide a quick diagnosis and a guide of releasing for unstable hemodynamics. A glance on mediastinum by video in VATS operations also provides early diagnosis and management. A postoperative X-ray is stronglyrecommended, because a small laceration in carina may lead to contralateral pneumothorax as well.
Conclusion
Accidental tracheobronchial injuries following endobronchial catheter insertion is unpreventable.We presented this case with unexplained hypotension and images to demonstrate a concealed pneumomediastinum as a midway to disaster tension pneumothorax.
REFERENCES
1.
Yüceyar L, Kaynak K, Cantürk E, Aykaç B. Bronchial rupture with a left-sided polyvinylchloride double-lumen tube. Acta Anaesthesiol Scand 2003;47(5):622–5. [CrossRef]
[Pubmed]

2.
Tezel C, Okur E, Baysungur V. Iatrogenic tracheal rupture during intubation with a double-lumen tube. Thorac Cardiovasc Surg 2010;58(1):54–6. [CrossRef]
[Pubmed]
3.
Gilbert TB, Goodsell CW, Krasna MJ. Bronchial rupture by a double-lumen endobronchial tube during staging thoracoscopy. Anesth Analg 1999;88(6):1252–3. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ying-Tzu Li - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Po-Yuan Shih - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ya-Jung Cheng - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Ying-Tzu Li et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}