 |
Case Report
Laparoscopic repair of subxiphoid hernia post-CABG repair
1 Associate Lecturer, General Surgical Department, University of Queensland, QLD, Australia
Address correspondence to:
Bertrand Ng Ren Joon
116 Water Street, South Toowoomba, QLD 4350,
Australia
Message to Corresponding Author
Article ID: 100066Z12BJ2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Joon BNR, Arafat Y. Laparoscopic repair of subxiphoid hernia post-CABG repair. J Case Rep Images Surg 2019;5:100066Z12BJ2019.ABSTRACT
Subxiphoid hernia as a complication of coronary artery bypass graft (CABG) surgery is uncommon. Coronary artery bypass graft subxiphoid hernia mainly occurs in patient who is elderly, high body mass index (BMI) and who has a lot of multiple comorbidities that can impact on healing. However, there are limited studies on the best approach to manage subxiphoid hernia; be it open or laparoscopic and the multiple variants of techniques being described. Due to its anatomic location, repairing subxiphoid hernia can sometimes posed difficulty to the most experienced surgeon, furthermore with a high complication rate. I present a case that I have gathered in a regional hospital who had a laparoscopic repair with a prosthetic mesh placed intraperitoneally (IPOM).
Keywords: Laparoscopic repair, Post-CABG, Subxiphoid hernia
Introduction
Subxiphoid hernia post-median sternotomy surgery has approximately 1–4.2% occurrence [1]. It is more common in male and the size of the hernia is usually small. In some cases, it can have multiple defects and asymptomatic. Hence, they usually do not seek medical attention. Subxiphoid hernia as a complication of CABG is uncommon. However, CABG surgery was first introduced in 1960s and we are seeing a good amount of cases that present with incisional hernia post-CABG surgery. I will present to you a case of laparoscopic repair subxiphoid hernia with a prosthetic mesh placed intraperitoneally (IPOM).
Case Report
A 75-year-old man, was seen in the surgical outpatient clinic, presented with a growing lump in the subxiphoid region post-CABG in 2014. He first noticed a lump over his previous sternotomy scar five years ago. It initially started as a small lump and had since grown gradually up to a size of 6 × 5 cm in the last five years. Despite being asymptomatic without any pain, the patient was very keen for it to be repaired as it is a hindrance for him to carry out his daily function with a huge lump on his chest and being cosmetically unpleasant. His subxiphoid hernia is reproducible whenever he coughs or sneezes however it is still reducible. He has denied any subxiphoid hernia prior to the CABG operation and has no previous abdominal and thoracic operation prior to the CABG operation. His other comorbidities include a BMI of 38.5 and Type 2 diabetes mellitus on oral hypoglycemic agents.
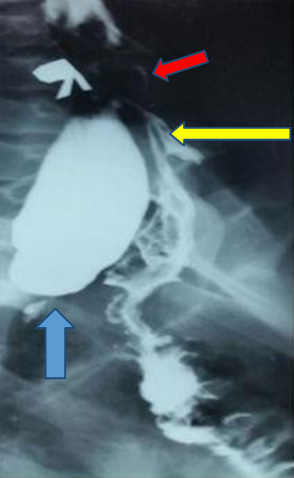
A computed tomography (CT) scan of the abdomen and pelvis was done two years ago and a defect was seen measuring approximately 6 × 3 cm with only fat content. There were no bowel loops seen in the sac and there was no diaphragmatic hernia noted (Figure 1, Figure 2).
He underwent a laparoscopic incisional subxiphoid hernia repair. Access to the abdominal cavity was achieved via an open Hasson technique with a 12 mm trocar with the initial incision done infraumbilically. Another 2 × 5 mm port was inserted on the left side of the hernia under direct vision (Figure 3). Photos were taken intraoperatively (Figure 4, Figure 5, Figure 6, Figure 7). Intraoperatively the hernia defect was measured to be approximately 6 × 5 cm in the longitudinal and transverse axis. Falciform ligament was taken down for adequate exposure with a diathermy. A composite polypropylene mesh of 20 × 15 cm with an anti-adhesive barrier was placed intraabdominally via the 12-mm trocar. The hernia sac was dissected out, however, the defect of the hernia was not closed. Dissection of the peritoneum was done to allow for exposure of the retro-xiphoid space for adequate overlap of the mesh. Nylon transfacial sutures were placed at the four corners of the mesh to keep the mesh elevated over the abdominal wall. They were retrieved with a laparoscopic Endoclose device on the preestablished skin site. The mesh was also reinforced with 5 mm helical tacks inferiorly, laterally, and as superiorly as the costal margin. Care was taken while using the tacks over the superior edge and costal margin to avoid the pericardium, diaphragm, and injuries to the intercostal nerve and vessel. The tacks were placed with a double crown technique. Postoperative patient was well and was discharged two days later with adequate analgesics.
On further follow-up at one month, the patient complained about a fluctuant mass around his subxiphoid area and further CT scan showed that the subxiphoid hernia had recurred.







Discussion
Subxiphoid hernia post-CABG repair mainly occur in the caudate position of the sternotomy scar as this is where the incision enters the epigastrium region of the abdomen. The weakness in the epigastric area compounded with lateral traction forces on the abdominal wall contributed to subxiphoid hernia occurring. The risk factors for subxiphoid incisional hernia includes, male, elderly (>65 years of age), obesity, previous median sternotomy wound infection, connective tissue disease, such as Marfan syndrome and Ehlers–Danlos syndrome, renal failure, protein or Vitamin C deficiency, immunosuppressed, smoking, and other treatments, such as corticosteroids and chemoradiotherapy [2],[3]. It is also deemed that in those who developed incisional hernia, there are a high numbers of those who has diabetes, arterial hypertension, and dyslipidemia [4]. Due to the location of a xiphoid hernia being below the diaphragm, bordered by the liver and falciform ligament and its close proximity to the ribs and the central tendon, repairing it has always been difficult. The main principle of hernia with mesh is ensuring wide overlap of at least 5 cm in all directions [5]. Ensuring adequate exposure with the need to take down falciform ligament and the dissection of retroxiphoid space to allow for the mesh to be placed have all been thought to improve surgical outcome and reduce recurrence rate [6].
Up to this point, only a limited number of studies can be found on subxiphoid hernia repair with most of it being limited by short follow-up time. Some studies recommend no fixation of superior part of the prosthesis while just fixing the inferior part of the mesh leaving stomach, liver, and intra-abdominal pressure to help protect the upper area, recommend using fibrin adhesions, while other studies recommend using combination of: closure of hernia defects with suture, use of relaxing incision on musculature and aponeurosis, and usage of surgical mesh to help prevent recurrence [4],[7]. An open approach with retromuscular/sublay mesh insertion which has been used in the last decades has shown to have a recurrence rates as high as 50% in some serial studies [7]. The laparoscopic approach does not diminish the recurrence rate but does result in less postoperative pain, better cosmetic results, shorter postoperative stay and recovery time [7]. Laparoscopic approach has been used in this case as it allows excellent subfascial visualization in the epigastric and edges of the defect, avoid previous incision site, minimize tissue trauma, reduce postoperative hospital stay [2].
Conclusion
Post-CABG xiphoid hernia mainly occurs in patient who is elderly, high BMI, and has a lot of multiple comorbidities that can impact on healing. Up to this point, there are limited number of studies done on approaches to subxiphoid hernia repair, and hence the best approaches and techniques to repair it are still far from sight. I present to you a case that I have gathered in a regional hospital that had a laparoscopic repair with a prosthetic mesh placed intraperitoneally (IPOM). Unfortunately, the patient had developed a recurrence of the hernia at one month follow and, hence, the technique that I described in the case report above may need further modification. As the number of patients with subxiphoid hernia post-CABG is raising, more prospective/retrospective studies should be done on subxiphoid hernia repair and patients should be followed up for short and long term to assess recurrence to determine the best approach.
REFERENCES
1.
Kim HS, Kim KB, Hwang HY, Chang HW, Park KJ. Subxiphoid incisional hernia development after coronary artery bypass grafting. Korean J Thorac Cardiovasc Surg 2012;45(3):161–5. [CrossRef]
[Pubmed]

2.
Shah HK, Chaudhari N, Khopade S, Thombare B, Chavan SG. Single incision Laparoscopic repair of post CABG sternotomy sub xiphoid hernia. J Minim Access Surg 2013;9(4):187–9. [CrossRef]
[Pubmed]
3.
Sanders DL, Kingsnorth AN. The modern management of incisional hernias. BMJ 2012;344:e2843. [CrossRef]
[Pubmed]
4.
de Mesquita GHA, Iuamoto LR, Suguita FY, et al. Simple technique of subxiphoid hernia correction carries a low rate of early recurrence: A retrospective study. BMC Surg 2017;17(1):51. [CrossRef]
[Pubmed]
5.
Conze J, Prescher A, Kisielinski K, Klinge U, Schumpelick V. Technical consideration for subxiphoidal incisional hernia repair. Hernia 2005;9(1):84–7. [CrossRef]
[Pubmed]
6.
Eisenberg D, Popescu WM, Duffy AJ, Bell RL. Laparoscopic treatment of subxiphoid incisional hernias in cardiac transplant patients. JSLS 2008;12(3):262–6.
[Pubmed]
7.
Suárez Grau JM, Bellido Luque JA. Advances in Laparoscopy of the Abdominal Wall Hernia. 1ed. London: Springer-Verlag; 2014. p. 159–81.
SUPPORTING INFORMATION
Author Contributions
Bertrand Ng Ren Joon - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yasser Arafat - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsI would like to express my deepest appreciation to the patient for allowing us to use his details.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Bertrand Ng Ren Joon et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}