 |
Case Report
First presentation of metastatic lung cancer as groin necrotizing fasciitis
1 MBBS, M. Surg (Sydney), Clinical Lecturer, University of Tasmania, Launceston General Hospital, Launceston, Tasmania, Australia
Address correspondence to:
Christopher Cheong
MBBS, M. Surg (Sydney), Clinical Lecturer, University of Tasmania, Launceston General Hospital, Launceston, Tasmania,
Australia;
Message to Corresponding Author
Article ID: 100119Z12CC2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cheong C. First presentation of metastatic lung cancer as groin necrotizing fasciitis. J Case Rep Images Surg 2023;9(1):17–19.ABSTRACT
Introduction: A B is a 64-year-old female who presented to the emergency department with fever, chill, and a swollen tender lump in the groin. She had a high white cell count of 14.0 × 109/L and a C-reactive protein (CRP) of 190 mg/L. She proceeded to have an urgent computed tomography (CT) scan.
Case Report: A B had a past medical history of poorly controlled diabetes (HbA1c = 11%) which she was non-compliant to medication. She also had an 80-pack year smoking history. A CT scan performed showed severe cellulitis with a collection with a suggestion of necrotizing fasciitis. She was taken to theater urgently for debridement. Histological examination of the debrided tissue however showed poorly differentiated adenocarcinoma which was consistent with metastatic lung adenocarcinoma.
Conclusion: This is the first case recorded of lung cancer with metastasis to the groin and presenting as a necrotizing soft tissue infection.
Keywords: Lung adenocarcinoma, Lung cancer, Metastasis, Necrotizing fasciitis, Poorly differentiated
Introduction
A B is a 64-year-old female who presented to the emergency department with fever, chill, and a swollen tender lump in the groin. She had a past medical history of poorly controlled diabetes (HbA1c = 11%) which was noncompliant to medication. A B also had an 80-pack year smoking history and was a current smoker. During her presentation, her blood tests revealed that she had a high white cell count of 14.0 × 109/L and a C-reactive protein (CRP) of 190 mg/L. A B then proceeded to have an urgent CT scan which showed severe cellulitis with a collection and a suggestion of necrotizing fasciitis. (Figure 1A and Figure 1B). Given her age and risk factors for necrotizing soft tissue infections A B was taken urgently to the operating theater for a debridement [1].

Case Report
Operative findings were that of necrotic tissue with pus in the groin crease that was debrided back to healthy tissue. A wound vacuum system was applied at the end of the case [vacuum-assisted closure (VAC) dressing].
The tissue was sent for histology which revealed poorly differentiated adenocarcinoma that on immunohistochemistry (IHC) showed TTF 1 positive, AE1/AE3 positive, S100 negative, PAX 8 negative. Programmed cell death ligand 1 (PD-L1) was also measured for the tumor and was 50%. This was consistent with metastatic lung cancer. The culture of the tissue did not grow any organisms.
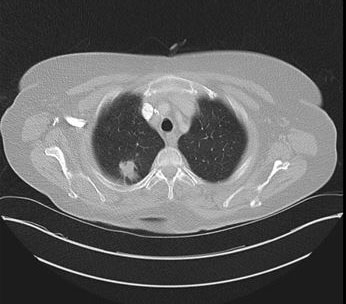
A completion CT brain/chest/abdomen was ordered which showed a lesion in right upper lobe apical segment which measures about 26 × 20 mm × 32 mm consistent with lung cancer (Figure 2). There were also hepatic, splenic, intracranial, multiple axial skeletal metastases.
A B was referred to the palliative care team as she did not want to see any active treatment.
Discussion
Worldwide more than 1 million people die of lung cancer each year. Lung cancer is 15–30 times more common in smokers than non-smokers [2]. Although it is known that smoking increases lung cancer, the pathogenesis of it is still poorly understood [2].
Lung adenocarcinoma is the most common primary lung cancer, accounting for 40% of lung cancers. Lung adenocarcinoma falls under the umbrella of non-small cell lung cancer (NSCLC) which are the most common in smokers [3]. The other variety of lung cancer is small cell lung cancer (SCLC).
Non-small cell lung cancer commonly metastasizes to the bone, liver, and the contralateral lung. In what is termed as distant organ metastasis or extrathoracic metastasis [4]. Patients with bone and liver metastasis from lung cancer often show poorer prognosis as compared to nervous system metastasis [5].
In patients with metastatic or stage IV NSCLC, the average survival rate at the five year mark is around 8%, with most patients surviving an average of six months from the date of diagnosis. However, there is a large spread on post-diagnosis survival times (ranging from three months to ten years) [6]. In patients with stage IV lung cancer, surgical resection is often not recommended as there is disseminated cancer. The current standard of care for these patients is platinum-based chemotherapy ± radiotherapy [6].
A review of the literature shows only one case report of metastatic lung cancer presenting with enlarged inguinal lymph nodes [7]. Inguinal metastases are highly unusual as the lymphatic system of the lungs do not drain to the inguinal nodes. As such the metastasis in this case is thought to be vascular in nature.
However, our case presented here is the only reported case of groin necrotizing soft tissue infection as the initial presentation of metastatic lung adenocarcinoma.
Conclusion
In conclusion, we report a rare case of groin necrotizing fasciitis and the initial presentation of metastatic lung cancer. This is a rare entity but however should remain a possible differential diagnosis.
REFERENCES
1.
Khamnuan P, Chongruksut W, Jearwattanakanok K, Patumanond J, Yodluangfun S, Tantraworasin A. Necrotizing fasciitis: Risk factors of mortality. Risk Manag Healthc Policy 2015;8:1–7. [CrossRef]
[Pubmed]

2.
Walser T, Cui X, Yanagawa J, et al. Smoking and lung cancer: The role of inflammation. Proc Am Thorac Soc 2008;5(8):811–5. [CrossRef]
[Pubmed]
3.
Myers DJ, Wallen JM. Lung Adenocarcinoma. 2023 Jan 29. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
[Pubmed]
4.
Acar P, Unsal M, Altintas N. Evaluation of lung cancer patients with distant organ metastasis. European Respiratory Journal 2014;44(Suppl 58):P2726.
5.
Riihimäki M, Hemminki A, Fallah M, et al. Metastatic sites and survival in lung cancer. Lung Cancer 2014;86(1):78–84. [CrossRef]
[Pubmed]
6.
Guo H, Li H, Zhu L, Feng J, Huang X, Baak JPA. “How Long Have I Got?” in Stage IV NSCLC patients with at least 3 months up to 10 years survival, accuracy of long-, intermediate-, and short-term survival prediction is not good enough to answer this question. Front Oncol 2021;11:761042. [CrossRef]
[Pubmed]
7.
Kanchustambham V, Saladi S. Adenocarcinoma of the lung with inguinal lymph node metastasis. Cureus 2021;13(3):e13658. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Christopher Cheong - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2023 Christopher Cheong. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}