 |
Case Report
Giant hiatal hernia: A review of the clinical presentation, surgical technique, and operative video
1 General Surgery, Université Catholic de Louvain, Louvain-la-Neuve, Belgium
2 General Surgery, Europe Hospitals, Brussels, Belgium
Address correspondence to:
Océane Wautelet
Chaussée de Louvain 718, 53, 1030 Schaerbeek,
Belgium
Message to Corresponding Author
Article ID: 100120Z12OW2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Wautelet O, Belle KV, Terryn FX. Giant hiatal hernia: A review of the clinical presentation, surgical technique, and operative video. J Case Rep Images Surg 2023;9(1):20– 24.ABSTRACT
Introduction: Giant hiatal hernia represents 0.3–15% of all hiatal hernia. Its complication such as the strangulation of the stomach are life-threatening. Therefore, in most of the cases it must be surgically handled.
Case Report: We report the case of a 74-year-old patient with giant hiatal hernia. He presented with sub-acute symptoms (e.g., vomiting, appetite loss, and hematemesis). Considering the symptomatology and complementary tests, we decided to perform a laparoscopic hernia repair using mesh reinforcement. We provided a commented operative video to describe the surgical procedure. We then discussed the surgical technique and decided how to conduct a safe and efficient repair.
Conclusion: A surgical approach is the recommended treatment in most giant hiatal hernia due to its life-threatening complications. The technique should be tailored to the patient. Although there is no consensus whether to use a mesh reinforcement, we believed that a cautious mesh placement should be considered when the crura are of poor quality. Surgeons should also be cautious with the fundoplicature and the risk of stricture, therefore we propose the systematic use of a tube to test the passage in the esophago-gastric junction.
Keywords: Hiatal hernia, Mesh reinforcement, Repair
Introduction
Hiatal hernia is a common pathology and its prevalence in the western population is estimated between 15% and 20% [1]. A giant hiatal hernia includes at least half of the stomach in the chest (or 30% depending on the author). Giant hiatal hernia represents 0.3–15% of all hiatal hernias [2]. The symptoms generally include pain, heartburn, regurgitation, dysphagia, cough, dyspnea, vomiting, and anemia. The main risk is incarceration and strangulation of the stomach, which is a rare but life-threatening complication. Hemorrhage is also a risk. Therefore, this type of hiatal hernia should generally be surgically handled. Based on this case report, we would like to review the surgical technique to conduct a safe and efficient repair.
Case Report
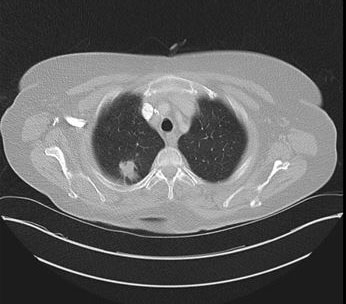
We report the case of a 74-year-old male patient who presented with vomiting, appetite loss, and hematemesis for ten days. A gastroscopy performed two weeks earlier showed grade A esophagitis and a mixed hiatal hernia with sliding and para-esophageal components. We performed another gastroscopy on arrival at the emergency room, which showed grade D esophagitis and a stomach located almost entirely in the thorax. There also was an important alimentary stasis. The CT scan displayed an intra-thoracic stomach positioned on the right side of the chest (Figure 1). From the upper gastrointestinal series, we can clearly see that two-thirds of the stomach are intra-thoracic, with an important dilatation of the esophagus associated (Figure 2). Considering the symptomatology, we decided to perform a laparoscopic hernia repair.
During the procedure, we first reduced the hernia and reinserted the stomach in the abdomen. We then thoroughly opened the hernia sac and released the stomach from it completely. We closed the esophageal hiatus with two sutures, using a polyester non-absorbable suture. We then reinforced the hiatal closure using a V-shaped polyester mesh coated on one side with collagen tissue. The mesh was fixed to the crura with three sutures. The branches of the V-shaped mesh were placed laterally so that there was no contact with the esophagus. Since the vascularization was already compromised by the reduction of the hernia, we tried to create an anti-reflux valve using the Nissen Rosetti technique, which preserves the short vessels. However, we suspected that there was some stricture, as we could not insert a nasogastric tube (36 Fr) through the esophago-gastric junction. Therefore, we dismantled the valve and made an anti-reflux fundoplication using the Dor anterior fundoplication technique.
We provide a commented surgical video (Video 1 ) to describe this surgical procedure. The patient went through a quick recovery. The upper gastrointestinal series on postoperative day 2 detected no recurrence nor sign of dysphagia (Figure 3). The patient was discharged on the third day after the intervention. The Dindo-Clavien classification was I.
One month later, the patient showed no signs of complication, no dysphagia, no more reflux symptoms and could eat normally.


Access video on other devices

Discussion
The repair of giant hiatal hernia is technically challenging and controversial. The laparoscopic approach has proven to be safe and reduces morbidity [3]. It seems that a tension-free reduction of the herniated stomach and excision of the hernia sac are key steps to reduce the risk of recurrence. However, there are some controversies around the use of mesh to reinforce the crural closure. Moreover, the debate also continues on the type of mesh that should be used. Rause et al. conducted a systematic review and network meta-analysis in October 2021, their results were based on the analysis of 17 articles with 1857 patients. Their analysis demonstrated a significant reduction of recurrence in patient with mesh reinforcement; however, it seems that there is still not enough evidence to assess the different mesh compositions [4]. This result was concordant with the systematic review of Furnée et al. which indicated a better outcome in terms of recurrence with mesh repair. They also pointed out that there are many kinds of meshes available and that there was a lack of randomized controlled studies to assess the most effective ones [5].
In 2020, Watson et al. conducted a double-blind controlled trial to compare the repair of large hiatus hernia with suture versus absorbable mesh versus non-absorbable mesh. They enrolled 126 patients. The long-term follow-up to five years showed similar outcomes in terms of recurrence, but the symptoms seemed to be worse after absorbable mesh repair (at three months: more heartburn and nausea, more odynophagia at one month, wheezing at six months and more inability to belch at 12 months follow-up) [6].
In our patient, the hiatus was large and the crura were thin, so we decided to reinforce the repair with a non-absorbable mesh. The tension on the repair was too high for a crura of poor quality and a cruroplasty alone would not have been strong enough to keep the hiatus closed. Laxague et al. tried to assess the use of a mesh in their systematic review [7]. Although they do not support the routine use of mesh during laparoscopic hiatal hernia repair, they also point out that, in case of large hiatus and poor quality of the crura, mesh repair could be beneficial.
The main complication occurring when using mesh repair is the erosion of the esophagus. However, those cases were mainly reported in case reports, which makes it difficult to assess its incidence. Li et al. conducted a systematic review which highlighted that we should keep an eye open for the complication when using mesh repair, especially in recurrent hernia. In addition, the mesh should be placed to maintain a safe distance from the esophagus [8]. Some authors also find that we should use U- or V-shaped prosthesis, which seems to have a lower risk than the use of a circular shaped mesh [4]. However, there is not enough evidence to promote a specific shape, so the choice remains the surgeon’s [9].
In our case, we believed that the risk of recurrence without mesh repair was higher than the risk of mesh erosion. We were also extremely cautious when placing the mesh to avoid any contact with the esophagus. In our case, the mesh was also coated with a collagen-based film on one side, to try and reduce tissue attachment.
The surgical technique for hiatal hernia repair classically includes fundoplication. In 2016, Fuzeng et al. compared the Nissen, Toupet, and Dor techniques. The reflux status was significantly improved in the three groups; however, Dor and Nissen techniques seemed better than Toupet in reducing the number of reflux episodes, long reflux, and the incidence of postoperative dysphagia [10]. In our case, we planned to do a “Nissen Rosetti” fundoplication, which preserves the short vessels (Figure 4). Indeed, the vascularization of the stomach was compromised by the reduction of the hernia; therefore, we did not want to reduce it more. The fundoplication was done using a calibration tube 36 Fr. However, the tube could not easily be inserted inside the lower esophagus. Therefore, we decided to undo the fundoplication and to convert it into a Dor fundoplication. The tube was then easily passed through the lower esophagus. Dysphagia is a well-known side effect following fundoplication. In 2005, Triponez et al. compared symptoms in patients who underwent laparoscopic fundoplication, patients with an incidentally discovered hiatal hernia, and a control group [11]. Although the fundoplication group had better reflux scores, they significantly presented more dysphagia. It is important to try to reduce this side effect to a minimum. Therefore, we systematically test the passage through the lower esophagus after fundoplication with a 36 Fr rigid plastic tube. If there is any resistance, we suggest dismantling the fundoplication.

Conclusion
Giant hiatal hernia repair is a rare and challenging pathology. Its consequences can be life-threatening and, therefore, a surgical approach is recommended. The choice of the surgical technique should be adapted to the patient’s condition. However, there are some key elements including a thorough reduction of the hernia and resection of the sac. When the hiatus is important and the crura are of poor quality, we believe that mesh reinforcement should be considered. The placement of the mesh must be cautious to reduce the risk of esophageal erosion. The choice of the mesh still belongs to the surgeon because of the lack of proof of the superiority of a type of mesh over another. Surgeons should also be cautious with fundoplication. To avoid stricture of the lower esophagus and reduce the risk of dysphagia, we suggest to systematically test the passage with a tube.
REFERENCES
1.
Dunn CP, Patel TA, Bildzukewicz NA, Henning JR, Lipham JC. Which hiatal hernias need to be fixed? Large, small or none? Ann Laparosc Endosc Surg 2020;5:29. [CrossRef]

2.
Mitiek MO, Andrade RS. Giant hiatal hernia. Ann Thorac Surg 2010;89(6):S2168–73. [CrossRef]
[Pubmed]
3.
Prassas D, Rolfs TM, Schumacher FJ. Laparoscopic repair of giant hiatal hernia. A single center experience. Int J Surg 2015;20:149–52. [CrossRef]
[Pubmed]
4.
Rausa E, Manfredi R, Kelly ME, et al. Prosthetic reinforcement in hiatal hernia repair, does mesh material matter? A systematic review and network meta-analysis. J Laparoendosc Adv Surg Tech A 2021;31(10):1118–23. [CrossRef]
[Pubmed]
5.
Furnée E, Hazebroek E. Mesh in laparoscopic large hiatal hernia repair: A systematic review of the literature. Surg Endosc 2013;27(11):3998–4008. [CrossRef]
[Pubmed]
6.
Watson DI, Thompson SK, Devitt PG, et al. Five year follow-up of a randomized controlled trial of laparoscopic repair of very large hiatus hernia with sutures versus absorbable versus nonabsorbable mesh. Ann Surg 2020;272(2):241–7. [CrossRef]
[Pubmed]
7.
Laxague F, Sadava EE, Herbella F, Schlottmann F. When should we use mesh in laparoscopic hiatal hernia repair? A systematic review. Dis Esophagus 2021;34(6):doaa125. [CrossRef]
[Pubmed]
8.
Li J, Cheng T. Mesh erosion after hiatal hernia repair: The tip of the iceberg? Hernia 2019;23(6):1243–52. [CrossRef]
[Pubmed]
9.
Granderath FA, Carlson MA, Champion JK, et al. Prosthetic closure of the esophageal hiatus in large hiatal hernia repair and laparoscopic antireflux surgery. Surg Endosc 2006;20(3):367–79. [CrossRef]
[Pubmed]
10.
Su F, Zhang C, Ke L, et al. Efficacy comparison of laparoscopic Nissen, Toupet and Dor fundoplication in the treatment of hiatal hernia complicated with gastroesophageal reflux disease. [Article in Chinese]. Zhonghua Wei Chang Wai Ke Za Zhi 2016;19(9):1014–20.
[Pubmed]
11.
Triponez F, Dumonceau J-M, Azagury D, et al. Reflux, dysphagia, and gas bloat after laparoscopic fundoplication in patients with incidentally discovered hiatal hernia and in a control group. Surgery 2005;137(2):235–42. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Océane Wautelet - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Koenraad Van Belle - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
François-Xavier Terryn - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementThere is no identifiable information, the anonymity of the patient is therefore preserved.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Océane Wautelet et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}