 |
Case Report
A rare case of metachronous bilateral noninvasive breast cancer with unilateral apocrine breast cancer diagnosed by preoperative core needle biopsy: A case report
1 Takahashi Breast and Gastroenterology Clinic, Osaka, Japan
Address correspondence to:
Keiichi Takahashi
Takahashi Breast and Gastroenterology Clinic, Yamazaki Seiren Bldg. 2F, 6-2-22, Uehonmachi, Tennoji-Ku, Osaka City, Osaka 543-0001,
Japan
Message to Corresponding Author
Article ID: 100167Z12KT2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Takahashi K. A rare case of metachronous bilateral noninvasive breast cancer with unilateral apocrine breast cancer diagnosed by preoperative core needle biopsy: A case report. J Case Rep Images Surg 2026;12(1):10–14.ABSTRACT
Introduction: Apocrine carcinoma of the breast is rare, accounting for 0.3% to 1% of all mammary gland malignancies. The incidence of bilateral breast cancer has been reported to range from 0.3% to 12% of all breast cancers. Furthermore, the incidence of synchronous bilateral carcinoma of the breast (SBC) is reported to be 1.0% of all breast cancers, while the incidence of metachronous bilateral carcinoma (MBC) of the breast is reported to be 7% of all breast cancers. Metachronous bilateral noninvasive cancer is even rarer, and few such cases have been reported to date. Metachronous noninvasive apocrine carcinoma of the breast developing in the contralateral breast after surgical treatment for ductal carcinoma in situ is extremely rare and has not been reported to date. This is the first report.
Case Report: The patient is a 73-year-old woman. A week ago, she noticed a lump in her left breast and visited the author’s clinic. The patient underwent right mastectomy and sentinel lymph node biopsy for right breast cancer five years ago. The histopathological result was ductal carcinoma in situ (papillary ductal carcinoma). After the subsequent five years without postoperative follow-up visits, she returned to the author’s clinic. On palpation, an elastic, hard mass approximately the size of 3.8-centimeter was palpable in the upper-outer quadrant and in the upper-inner quadrant of the left breast. Core needle biopsy (CNB) was performed. The results demonstrated apocrine breast cancer. More specifically, she had ductal cancer in situ (DCIS) with tumor cells showing apocrine features.
Conclusion: Apocrine breast cancer is a rare disease, and metachronous bilateral noninvasive breast cancer is even rarer and has not been reported to date. Here, a rare case of apocrine carcinoma of the breast is reported.
Keywords: Apocrine carcinoma of the breast, Metachronous bilateral carcinoma of the breast, Noninvasive cancer, Synchronous bilateral carcinoma of the breast
Introduction
The incidence of bilateral breast cancer is reported as 0.3% to 12% of all breast cancers [1], with the value for synchronous bilateral carcinoma of the breast (SBC) reported as 1.0% and metachronous bilateral carcinoma (MBC) of the breast as 7% of all breast cancers [2].
Apocrine breast cancer is a rare disease reportedly accounting for 0.3% to 1% of all breast cancers [3], and metachronous bilateral noninvasive breast cancer is even rarer and has not been reported to date. A case of bilateral noninvasive breast cancer with unilateral metachronous apocrine breast cancer, an extremely rare case, diagnosed by preoperative CNB is reported.
Case Report
The patient was a 73-year-old woman with a history of atrial fibrillation and hypertension after surgical treatment of uterine fibroids. She underwent right mastectomy and sentinel lymph node biopsy for right breast cancer five years ago. The histopathological results were as follows: ductal carcinoma in situ (papillary ductal carcinoma), pTis (8.3 × 4.3 cm), pN0 (sn 0/3), M0, pStage 0, ER 10%, PgR 0%, HER2 3+, Ki67 20%, and HG2. After the subsequent five years without postoperative follow-up visits, she noticed a lump in her left breast a week ago and visited the author’s clinic again. On palpation, an elastic, hard mass approximately the size of 3.8-centimeter was palpable in the upper-outer quadrant and in the upper-inner quadrant of the left breast. No enlarged axillary or supraclavicular lymph nodes were observed.
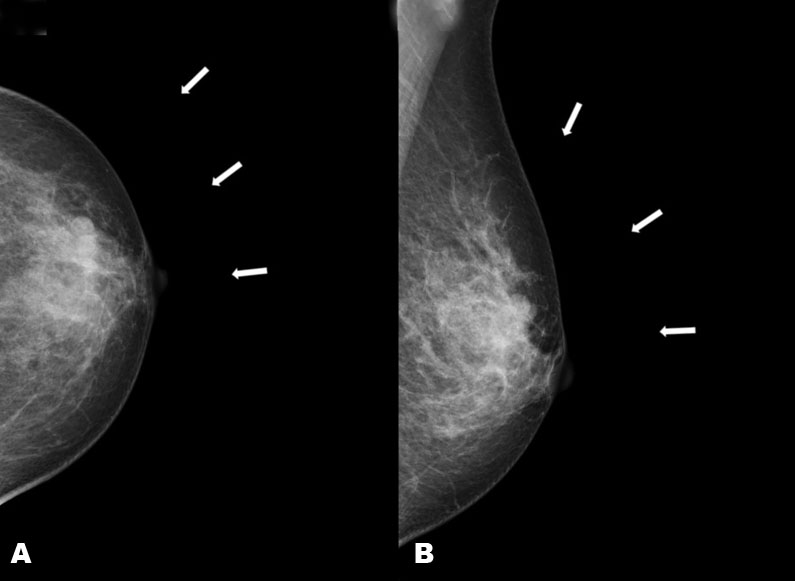
Mammography (MMG) revealed an irregular mass shadow measuring approximately 3.8 cm in the left M-O region of the breast (Figure 1A and Figure 1B).
Ultrasonography (US) revealed an irregular mass shadow measuring approximately measuring approximately the size of 3.8 cm in the upper-outer quadrant and in the upper-inner quadrant of the left breast. Color Doppler echo imaging showed a hypervascular pattern (Figure 2A and Figure 2B).
Core needle biopsy (CNB) was performed (Figure 2C and Figure 2D). The results demonstrated apocrine breast cancer.
Tumor cells were polygonal with densely stained nuclei and eosinophilic, granular, or vacuole-rich cytoplasm, proliferating in a solid manner and partly forming a ductal structure. Nuclear anisokaryosis was observed. These findings demonstrated DCIS with tumor cells showing apocrine features (Figure 3A and Figure 3B).
Computed tomography (CT) revealed an irregular area in the upper-outer quadrant and in the upper-inner quadrant of the left breast under contrast enhancement (Figure 4A and Figure 4B).
Magnetic resonance imaging (MRI) revealed non-mass enhancement in the upper-outer quadrant and in the upper-inner quadrant of the left breast (Figure 5).
The treatment plan was determined at a preoperative multidisciplinary conference attended by breast surgeons, radiologists, and pathologists.
Based on imaging tests such as MRI, the tumor was found to be 3.8 cm in size and had spread close to the nipple; therefore, a partial mastectomy was not an option, and a total mastectomy was selected. Although the preoperative CNB indicated noninvasive cancer, it is only after examining all sections of the postoperative specimen that it becomes clear whether the tumor consists entirely of noninvasive carcinoma and contains no invasive carcinoma. For this reason, it is desirable to combine this approach with sentinel lymph node biopsy to minimize the burden on the patient as much as possible.
Right mastectomy and sentinel lymph node biopsy were performed. The histopathological results were as follows: pStage 0 (TisN0M0), apocrine ductal carcinoma in situ (38 × 18 × 33 mm), high nuclear grade, margin-,pN0 (sn 0/4), ER−, PgR−, AR (androgen receptor) 80%, HER2−, and Ki67 5–10%.
The treatment plan for postoperative adjuvant therapy involved no adjuvant therapy because it was noninvasive cancer.
Follow-up observations two years after surgery show no signs of recurrence.




Discussion
The incidence of bilateral breast cancer is reported as 0.3% to 12% of all breast cancers [1], with the value for SBC reported as 1.0% and MBC as 7% of all breast cancers [2],[3].
Bilateral noninvasive breast cancer with metachronous apocrine breast cancer is extremely rare and has not been reported to date. Apocrine breast cancer is a rare disease reportedly accounting for 0.3% to 1% of all breast cancers [4]. The mean age of patients is 57.0 years, which is slightly higher than that of ordinary breast cancer.
Apocrine carcinoma of the breast is defined as a special histologic subtype of invasive carcinoma with dominant apocrine metaplasia. The WHO’s essential and desirable criteria define it as a tumor that exhibits apocrine morphology in more than 90% of tumor.
Clinically, apocrine carcinoma usually presents with a palpable tumor mass, rarely with a bloody discharge from the nipple or as a cyst [5],[6].
Histologically, apocrine carcinoma of the breast exhibits a ductal structure and is characterized by eosinophilic, granule-rich cytoplasm. Compared with benign apocrine metaplasia, apocrine carcinoma of the breast is characterized by larger nucleoli and more marked anisocytosis. This is a rare disease reportedly accounting for 0.3% to 1% of all breast cancers.
Apocrine carcinoma of the breast has no characteristic imaging findings compared with ordinary breast cancer. Most cases of ordinary noninvasive breast cancer are luminal type, while many cases of noninvasive apocrine carcinoma of the breast have the phenotype ER−, PgR−, and AR+ [7]. The positivity rate of HER2 is 30–60% [8],[9]. The risk of recurrence increases in cases with HER2 positivity [10] and high Ki67 [11]. Regarding prognosis, there is no difference in survival or recurrence rates compared with ordinary ductal carcinoma [12].
Conclusion
Apocrine breast cancer is a rare disease, and bilateral noninvasive breast cancer with metachronous apocrine breast cancer is even rarer and has not been reported to date. An extremely rare case of noninvasive apocrine carcinoma of the breast—namely, metachronous bilateral noninvasive breast cancer with unilateral rare apocrine breast cancer diagnosed by preoperative CNB—was reported.
REFERENCES
1.
Manea E, Munteanu A. Evolution of synchronous bilateral breast carcinoma in a young patient. Rev Med Chir Soc Med Nat Iasi 2016;120(1):192–6.
[Pubmed]

2.
Jobsen JJ, van der Palen J, Ong F, Riemersma S, Struikmans H. Bilateral breast cancer, synchronous and metachronous; differences and outcome. Breast Cancer Res Treat 2015;153(2):277–83. [CrossRef]
[Pubmed]
3.
Ramezani M, Amiri A, Kavousi F, Sadeghi M. Synchronous bilateral breast cancer (SBBC): Report of a case with review of literature. American Journal of Medical Case Reports 2017;5(12):301–3. [CrossRef]
4.
Dellapasqua S, Maisonneuve P, Viale G, Pruneri G, Mazzarol G, Ghisini R, et al. Immunohistochemically defined subtypes and outcome of apocrine breast cancer. Clin Breast Cancer 2013;13(2):95–102. [CrossRef]
[Pubmed]
5.
Mardi K, Sharma J, Sharma N. Apocrine carcinoma of the breast presenting as a solitary cyst: Cytological and histopathological study of a case. Indian J Pathol Microbiol 2004;47(2):268–70.
[Pubmed]
6.
Agoff SN, Swanson PE, Linden H, Hawes SE, Lawton TJ. Androgen receptor expression in estrogen receptor-negative breast cancer. Immunohistochemical, clinical, and prognostic associations. Am J Clin Pathol 2003;120(5):725–31. [CrossRef]
[Pubmed]
7.
Vranic S, Schmitt F, Sapino A, Costa JL, Reddy S, Castro M, et al. Apocrine carcinoma of the breast: A comprehensive review. Histol Histopathol 2013;28(11):1393–409. [CrossRef]
[Pubmed]
8.
Vranic S, Marchiò C, Castellano I, Botta C, Scalzo MS, Bender RP, et al. Immunohistochemical and molecular profiling of histologically defined apocrine carcinomas of the breast. Hum Pathol 2015;46(9):1350–9.
9.
Provenzano E, Gatalica Z, Vranic S. Carcinomas with apocrine differentiation. WHO Classification of Tumours Editorial Board, editor. WHO classification of breast. 5th ed. Lyon (France): IARC Press; 2019. p. 131–3.
10.
Guo W, Wang W, Zhu Y, Zhu X, Shi Z, Wang Y. HER2 status in molecular apocrine breast cancer: Associations with clinical, pathological, and molecular features. Int J Clin Exp Pathol 2015;8(7):8008–17.
[Pubmed]
11.
Yoshino R, Hatanaka N, Takahashi K, Ito A, Ujiie N, Yasuda S, et al. Clinicopathological features and prognostic factors of apocrine carcinoma of the breast in a cohort of 63 patients. Discov Oncol 2025;16(1):1743. [CrossRef]
[Pubmed]
12.
Abati AD, Kimmel M, Rosen PP. Apocrine mammary carcinoma. A clinicopathologic study of 72 cases. Am J Clin Pathol 1990;94(4):371–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Keiichi Takahashi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2026 Keiichi Takahashi. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}